All-on-4 dental implants are a full-arch rehabilitation technique that uses just four titanium implants — two placed axially in the anterior jaw and two placed at a posterior angulation of 30–45 degrees — to support a complete fixed bridge. Conceived and developed by Portuguese oral and maxillofacial surgeon Paulo Maló in collaboration with Nobel Biocare in the early 2000s, All-on-4 represented a paradigm shift in the treatment of edentulism: by tilting the posterior implants, surgeons could avoid the sinus cavities in the upper jaw and achieve a longer implant-to-bone contact surface without bone grafting in many cases. For patients across the UK seeking full mouth implants — and those exploring treatment in Turkey — All-on-4 remains one of the most evidence-based full-arch solutions available.
As a specialist prosthodontist, I assess each patient's suitability for All-on-4 against clinical and anatomical criteria, coordinate the UK-based consultation and diagnostic phases, and oversee prosthetic planning and delivery in collaboration with our experienced surgical team in Antalya. The combination of specialist prosthodontic expertise and the economic advantages of treatment in Turkey enables patients to access premium-quality full-arch rehabilitation at a fraction of typical UK pricing.
The All-on-4 Concept and Surgical Rationale
The engineering insight at the core of All-on-4 is biomechanical: the posterior angulated implants extend the effective support span of the prosthetic arch, reducing the cantilever forces that would otherwise be borne by fewer, shorter implants in a straight-line arrangement. This allows a full arch of 10–12 teeth to be supported stably on just four implants, even in jaws where the posterior bone is limited due to sinus pneumatisation or bone resorption.
Angulated Posterior Implants — Why Tilted at 30–45°
Placing the posterior implants at an angle of 30–45 degrees mesially serves several biomechanical purposes. First, the implant traverses a greater cross-sectional area of available bone, achieving longer osseointegration surface contact. Second, the implant apex emerges in denser, more coronal bone — typically in the D1 or D2 Misch classification — which supports reliable primary stability and early osseointegration. Third, in the upper jaw, angulation allows the implant to be positioned anterior to the maxillary sinus floor, entirely avoiding the need for sinus augmentation in the majority of cases. The angulation does introduce a prosthetic complexity: multi-unit abutments are used to redirect the prosthetic screw access from the angulated implant to a near-vertical path, ensuring clean screw-access openings in the bridge.
Immediate Loading Protocol
Immediate loading — attaching a provisional bridge on the day of surgery — is a defining feature of the All-on-4 protocol. This is only clinically appropriate when primary implant stability meets the required threshold, typically an insertion torque of 35 Ncm or greater. The provisional bridge is fabricated from PMMA acrylic resin and is adjusted to reduce occlusal loading, particularly in excursive movements. Patients are placed on a soft diet for approximately 12 weeks while osseointegration consolidates. The provisional phase is not merely a patient comfort measure — it also allows the clinician to refine the aesthetics, vertical dimension of occlusion, and phonetics before fabricating the definitive prosthesis.
Evidence Base
The All-on-4 protocol has been extensively studied. The landmark publication by Maló et al. (2011), a prospective study of 245 edentulous patients followed over 10 years, reported an implant survival rate of 94.8% in the mandible and 93.5% in the maxilla. Subsequent independent systematic reviews have confirmed these findings: Papaspyridakos et al. (2012) meta-analysis, examining 13 studies, reported a cumulative implant survival rate of 98.0% at a mean follow-up of 26.2 months. Patient-reported outcomes are equally compelling. Studies consistently document substantial improvements in the Oral Health Impact Profile (OHIP-14) scores, with patients reporting dramatic gains in chewing efficiency, self-confidence, and quality of life compared to their pre-treatment denture-wearing baseline.
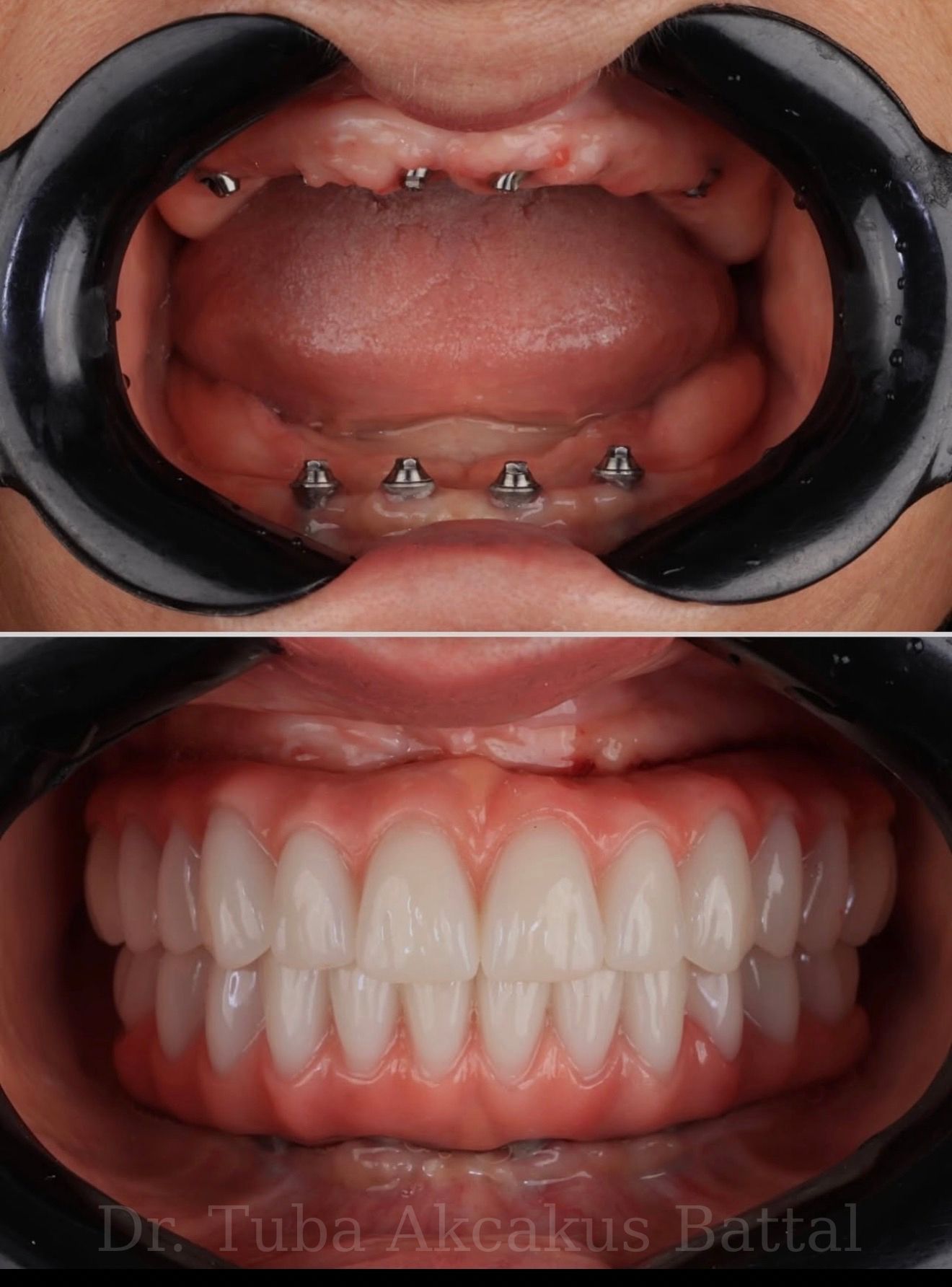
All-on-4 clinical result — full arch restored, natural aesthetics
All-on-4 vs All-on-6
Both protocols achieve full-arch fixed rehabilitation, but the choice between them depends on bone anatomy, occlusal load requirements, and clinical risk stratification. All-on-6 adds two posterior implants, reducing the cantilever length and distributing prosthetic stresses more evenly across the arch. This makes All-on-6 preferable in patients with strong parafunctional habits such as bruxism, in cases where posterior bone density is adequate, or where the patient has a longer face and wider arch requiring a more extended bridge span. All-on-4 is advantageous when posterior bone is limited, when the goal is to avoid bone grafting, or when the treatment needs to be completed in a single surgical stage without augmentation procedures.
Patient Selection: Who Qualifies?
All-on-4 is indicated for patients who are fully edentulous in one or both arches, or those with multiple non-restorable teeth requiring extraction. Borderline cases — patients with some remaining teeth of questionable prognosis — require careful discussion to determine whether extraction and All-on-4 is more appropriate than a mixed implant-and-conservation approach. The following criteria guide selection:
- Adequate anterior bone volume (minimum 10mm height, 6mm width in the anterior region)
- Controlled or absent systemic conditions that impair osseointegration (notably: uncontrolled diabetes is a contraindication; well-managed diabetes is generally acceptable)
- Non-smoker or committed to cessation perioperatively — smoking doubles the implant failure risk
- No active bisphosphonate use or recent history of radiation to the jaw
- Realistic expectations: patients should understand the provisional phase, dietary restrictions during healing, and the long-term maintenance commitment
Pre-surgical planning involves a CBCT scan and full clinical assessment. In the maxilla, the relationship between available bone height and the sinus floor is a key determinant of whether standard All-on-4 angulation is sufficient or whether additional procedures are needed. In the mandible, the position of the mental foramen defines the posterior limit of safe implant placement.
The Prosthetic Options: Hybrid Bridge Materials
Once osseointegration is confirmed, the definitive All-on-4 bridge can be fabricated from several material systems, each with distinct clinical trade-offs. Full-contour zirconia (Y-TZP) is the current clinical gold standard: with flexural strength exceeding 900 MPa, excellent biocompatibility, and resistance to staining and wear, it offers the longest projected service life. A titanium-reinforced acrylic hybrid bridge is lighter, more economical, and allows easier chair-side repairs, but the acrylic component is subject to wear and requires replacement typically within 5–8 years. Monolithic PMMA bridges are used for the provisional phase and are not intended as permanent restorations. For a full comparison of prosthetic materials used across implant-supported restorations, see our guide to dental crown and bridge materials.
Your Treatment Pathway: UK to Antalya
The pathway for UK patients seeking All-on-4 dental implants in Turkey begins with an online or in-person consultation with me in the UK. This initial appointment covers your full dental and medical history, review of any existing radiographs, a discussion of your goals and concerns, and the production of a detailed written treatment plan and cost estimate. No commitment is required at this stage.
For patients who proceed, the surgical phase takes place at our carefully selected partner clinic in Antalya. The city is a major centre for dental tourism, with well-equipped clinics operating to international standards and accredited by the Turkish Ministry of Health. Implant systems used are the same premium brands available in UK practices — Nobel Biocare, Straumann, and Osstem. The significant cost difference arises from Turkey's lower operational costs and currency differential, not from any reduction in clinical standards. Following surgery in Antalya, post-operative follow-up and coordination continues through my UK practice, ensuring a seamless continuum of care for healing monitoring, any prosthetic adjustments, and long-term maintenance.
Frequently Asked Questions
How many teeth do you get with All-on-4?
The All-on-4 bridge typically provides 10–12 prosthetic teeth per arch, delivering a full, aesthetically complete smile. The exact tooth count varies with the jaw width and bridge design — your treatment plan will specify the number of units included in your prosthesis.
Can All-on-4 fail?
As with all implant-based treatments, failure is possible but uncommon in well-selected patients following the correct protocol. The 10-year implant survival data reported by Maló et al. (2011) is 94.8%. The main risk factors for failure include smoking, uncontrolled systemic conditions (particularly diabetes), poor bone quality (D4 Misch classification), and inadequate post-operative care. Early failures — occurring within the first few weeks — are typically related to insufficient primary stability or infection. Late failures are more commonly associated with peri-implantitis resulting from inadequate hygiene.
What is recovery like after All-on-4?
Post-operative recovery involves swelling, bruising, and tenderness that typically peaks at 48 hours and resolves over 7–10 days. Prescribed analgesics (NSAIDs and paracetamol) manage discomfort effectively for most patients. Most people are able to resume light work within 3–5 days. A soft diet is maintained for 12 weeks to protect the healing implants. The provisional bridge allows normal social function and conversation immediately, but patients should avoid hard, crunchy, or chewy foods during the osseointegration period.
How does the cost compare between the UK and Turkey?
In the UK, All-on-4 treatment typically costs between £12,000 and £22,000 per arch depending on the implant system, prosthetic material, and the complexity of any pre-surgical procedures required. In Antalya, the same quality of treatment — using premium implant brands and full-contour zirconia — is available at 50–60% lower overall cost. With flights and accommodation in Antalya generally modest, patients typically save significantly even after accounting for travel, while receiving care coordinated by a UK-based prosthodontic specialist throughout.

All-on-4 — fixed teeth, natural smile